
Wednesday, October 29, 2003
3612
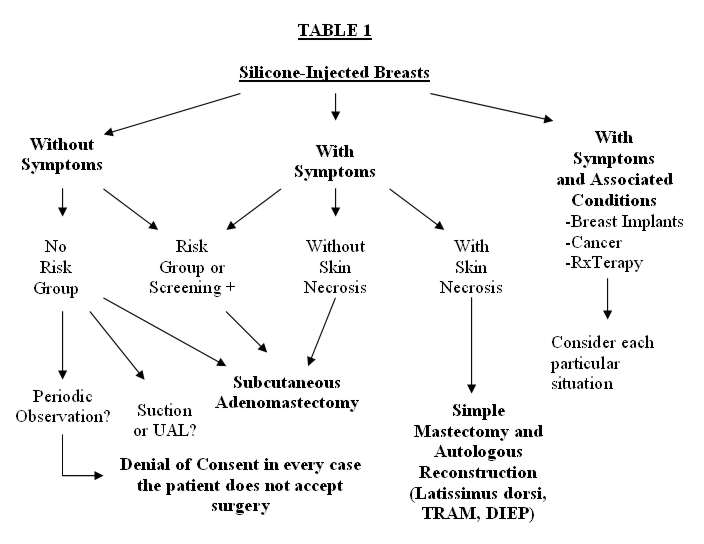
P23: Algorithm in Management of the Silicone-Injected Breast
Purpose: The injection of liquid silicone for breast augmentation leads to complications and controversial decisions regarding further treatment, difficult to accept in “healthy” patients (pts). This poster will present an algorithm to approach the management of silicone-injected breasts. We considered patients with and without symptoms. Our series includes cases with silicone injections and mammary implants, breast cancer and radiotherapy. Diagnosis, acceptance or refusal of treatment, the treatment itself and complications are discussed. Material and Methods: We studied 17 pts from March 2000-February 2003. The pts were divided into three groups: 1) without symptoms, n=9, 2) with symptoms, n=4, 3) with symptoms and associated conditions (breast implants, breast cancer, and radiotherapy), n=4, mean age: 27.3 years. Pts were considered to be in a risk group when they had family history of breast cancer or positive markers for BRCA1 or BRCA2. Results: Every patient was informed about the potential risks of local complications and chances to mask a breast cancer. However, patients with local complications (fistulae, skin necrosis, and hard lumps), 9 / 17(with and without symptoms) were reluctant to undergo any kind of surgical procedure. Diagnosis of these patients included: 1) mammogram and 2) MRI. Ultrasound is not very effective for detection but may help in some cases. The treatment’s algorithm is shown in Table 1. Three patients had breast prostheses inserted after the injection, and in one breast cancer was detected. Complications included: asymmetries, breast ptosis, skin involvement, silicone fistulae and skin retraction after radiotherapy. Conclusions: We reviewed a 17- patient series with silicone-injected breasts. Although many patients remain symptom-free for a long time, silicone migration is observed. In every case we indicate subcutaneous mastectomy in asymptomatic patients, and simple mastectomy with autologous reconstruction when there is any type of skin involvement. We never used suction or ultrasonic-assisted liposuction (UAL) in these cases, but UAL might be considered in cases of partial treatment of asymptomatic patients. Whenever patients decline surgery, we suggest them to sign a refusal of consent. Nine of 17 cases did not accept any kind of surgery even in cases of complications.
View Synopsis (.doc format, 66.0 kb)
See more of Posters
Back to Plastic Surgery 2003 Complete Scientific Program
Back to Plastic Surgery 2003 Meeting home